Sex, Orgasm, Drugs, Oxytocin, Arginine Vasopressin (AVP), Prolactin, Norepinephrine (Non-adrenaline), Epinephrine (Adrenaline), and Neuroplasticity –




(The pituitary gland and its 3 major hormones- Oxytoxin, AVP, and PRL structure from http://en.wikipedia.org)
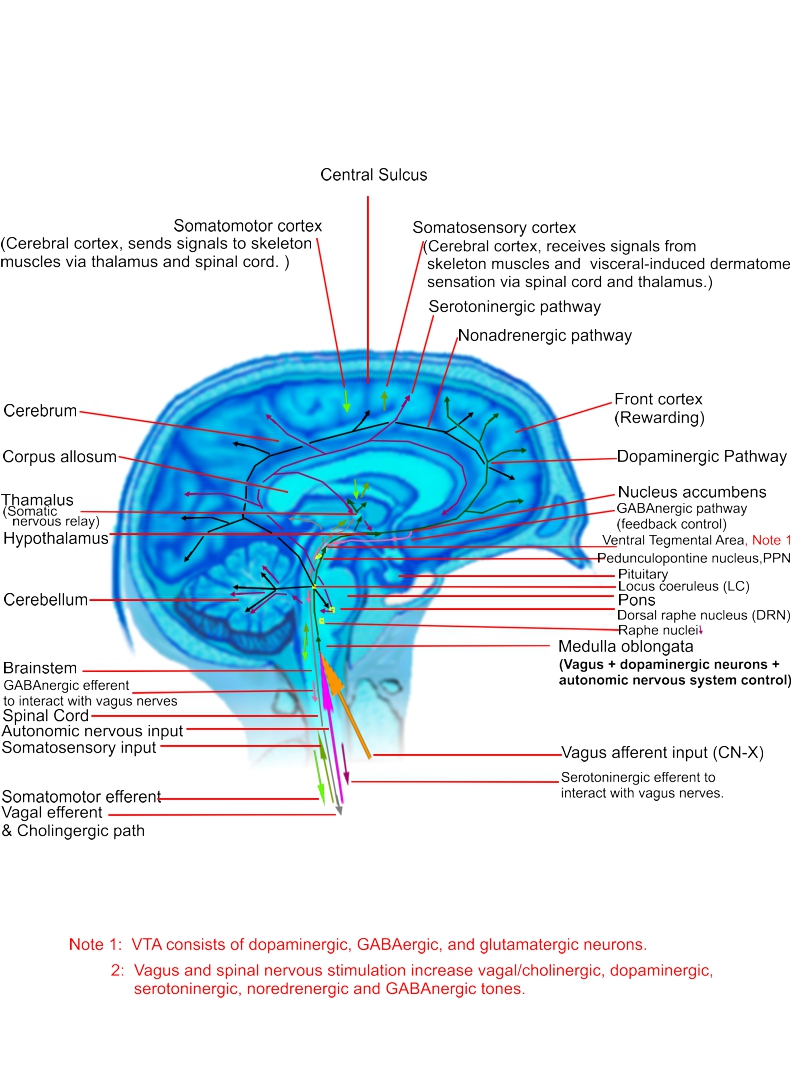
The syntheses of hormones and neurotransmitters induced by orgasm alternate the brain and neuroendocrine function and promote neuroplasticity for the central nervous system as well as peripheral nervous system, either sensory or motoring. Sexual activities not only bring innocence into adulthood in a short term (almost instant), but also let you become addictive to psychological attachment or/and physical pleasure for better or worse. Drug abuse usually alternates the central nervous system – dopaminergic, cholinergic, serotoninergic, GABAergic, noradrenergic and adrenergic, for worse. As matter of fact, sex is a powerful drug since it alternates the body function in few seconds and its effects can last in a few days or months, if not in minutes or hours. The duration of post-orgasm or post-ejaculation neuro-endocrine modification is called refraction time. The pituitary hormones oxytocin and prolactin play the key roles affecting the duration of refraction time. AVP is responsible for love-bonding after having sex. The orgasm desctructive effects are generated by persistent, excessive hypothalamic and adrenal dopamine-norepinpehrine (-epinephrine) conversion in the stress response axis – the hypothalamus-pituitary-adrenal axis, and its induced excessive prostaglandin E2 (or PGE2, for inflammation,carcinogenesis andfever; natural anti-PGE2 drug Resolvins: Omega-3 + (Aspirin or water willow‘s salicin)) and excessive histamine synthesis in the brain and all-over-body cells (http://action.love/WordPress/2013/07/31/orgasm-premature-ejaculation-and-histamine-receptors/) with continuous prolactin and norepinephrine release for arterial constriction that castrates the hypothalamus-pituitary-testicular (or ovarian) axis. Traditional Chinese Medicine (TCM) uses the term “Weak Kidney??” or “Kidney Qi Deficiency??” to describe the sex-induced destructive effects. Mixing sex with street drugs is even more destructive, and the resulted nervous destruction (negative neuroplasticity) may become irrecoverable.
Neuroplasticity refers to the adaptive ability of the brain to generate, reorganize or change neural pathways based upon new experiences. This special characteristic enables the brain to evolve through the life time by adding new neurons and memory cells, by eliminating unused neurons and memory cells, or by alternating neural communication pathways. This ability lets us lean new skills , memorize new things, recover from injury rehabilitation, adapt an new environment, or even train an old dog new tricks. Brain can be stimulated to increase its responsiveness and coordination by growing new synapses, strengthening existing synapses and by extending axons ( neuron cell bodies) from one area to another area. Synapses are the interconnection among neurons so that information can be passed from one neuron to others. A synapse consists of presynaptic and postsynaptic terminals, which are separated by a synaptic cleft. When a nervous signal, that is an electric pulse or action potential, is transduced from one neuron (presynaptic neuron) to the next one (postynaptic neuron), it excites the presynaptic terminal, filled with small vesicles containing chemical neurotransmitters to release the neurotransmitters to the postsynaptic terminal consisting of receptors specific for these neurotransmitters. Across the synaptic cleft, the neurotransmitters bind to receptors and produce an electrical pulse in the postsynaptic cells. The postsynaptic neuron may receive multiple inputs from different synapses that is, different presynaptic neurons. The postsynaptic neuron will fire an action potential if the sum of all its postsynaptic electrical pulses is over a voltage threshold for firing. Frequently repetitive exciting the synapses will grow the postsynaptic cells for neuroplasticity. For examples, martial art or boxing masters have trained their brain to react extremely fast in response to visual or auditory stimulation of an acting object.
Neuroplasticity also means nervous rejuvenation or regeneration. Neurons can be rerouted to enable functioning in a damaged part of the brain after a stroke or injury has occurred and to a transplanted heart. This bring s hope for the patients to restore their body function. A transplanted heart varies the heart beat in responses to exercises after the vagal and sympathetic nerves are relinked together.
Neuroplasticity also include the alternation of the genes involved neurotransmitter synthesis and of the gene expression (or sensitivity) of the receptors. Deficiency of neurotransmitters or under-expression of receptors may cause neuron death or synapse degeneration, while excess of neurotransmitters or over-expression of receptors may result in outgrowth of neurons and synapses. Prolonged excitation of a nervous system with drugs or practices results in adaptation of the receptors to their use. Receptors can increase or decrease in number and/or sensitivity to the neurotransmitter responsible for the nervous system, which is known as upregulation or downregulation, respectively. A larger dose of drugs or a higher-frequent practices may be needed to produce the same result; this phenomenon known as tolerance. Withdrawal of the drugs or practices can result in nervous receptor hypoactivity which produces symptoms known as withdrawal. The phenomenon of receptor adaptation leads to long-term memory or addiction, whichever is a result of neuroplasticity, Neuroplasticity is a double-edge sword, depending on its constructive or destructive effects on life.
Neurotransmitters are endogenous neurochemicals released from a neuron terminal or a stimulating receptor, acting as signal transmission messengers to transmit signals from a neuron or a stimulating receptor to a target cell or downstream neurons across a synapse. They are released under stimulation of a nervous voltage pulse such as action potential or a graded electrical potential induced by the local permeability of the neuron’s membrane to ions sodium (Na+), potassium (K+), chloride (Cl–), and/or calcium (Ca2+)). Low-level release of neurotransmitters can occur under ion diffusion across the membrane even without electrical stimulation. A weaker membrane will likely produce a higher grade electrical potential via ion diffusion. Neurotransmitters are stored in the synaptic vesicles of axon terminals on the presynaptic side of a synapse; after being released into the synaptic cleft,, they bind to receptors in the membrane on the postsynaptic side of the synapse, resulting in generation of an action potential for the next neuron, as nervous transduction, or in exertion of biologic effects on the receptors. A certain amount of neurotransmitters are reuptaken back to the pre-synaptic vesicles for reuse. Some may be diffused and metabolized (broken down) into the blood stream across the blood-nervous barriers, once they reach the post-synaptic neurons or effectors to prevent further excitatory or inhibitory signal transduction. There are several neurotransmitters and neurohormones participating in neuroplasticity. The main players are acetylcholine and norepinephrine which elicit the formation of long-term memory, addiction, or/and post-traumatic stress syndromes. Other neurotransmitters or neurohormones, such as dopamine, epinephrine, serotonin, GABA, Arginine Vasopressin (AVP), and endorphin also affect of long-term memory and play an important role in modulating the process of neuroplasticity.
Chronic stress causes the neuroplasticity of the hypothalamus and autonomic nervous control cells. The hypothalamus-pituitart-adrenal axis responds to stress by activating the paraventricular nucleus neurons – magnocellular neurosecretory cells and parvocellular neurosecretory neurons, to release neurohypophysial peptides, and by evoking the corticotropin-releasing hormone neurons, the limbic system, and the brainstem and spinal cord projecting neurons that regulate autonomic nervous system. Chronic stress leads to enhanced expression of secreted neuropetides, depressed expression of glucocorticoid receptors and GABA receptor subunits and enhanced glutamate receptor expression. Chronic stress induces morphological plasticity in paraventricular nucleus neurons, with a change in cell size and an alternation of GABAergic and glutamatergic innervation.
http://www.ncbi.nlm.nih.gov/pubmed/18655895
http://www.ncbi.nlm.nih.gov/pubmed/15240350
http://www.ncbi.nlm.nih.gov/pubmed/9023876
http://www.ncbi.nlm.nih.gov/pubmed/16271821
http://www.ncbi.nlm.nih.gov/pubmed/16647726
http://www.ncbi.nlm.nih.gov/pubmed/7621982
http://www.ncbi.nlm.nih.gov/pubmed/8264865
http://www.ncbi.nlm.nih.gov/pubmed/8597392
Neurotransmitters involved neuroplasticity
Acetylcholine is a neurotransmitter in both the peripheral nervous system (PNS) and central nervous system (CNS). The vagal neurons, pre- or post parasympathetic neurons, all preganglionic sympathetic neurons, pseudomotor neurons to sweat glands of the postganglionic sympathetic fibers , and the motor division of the somatic nervous system uses it as a neurotransmitter. Note that the sensory neurons of the somatic nervous system uses glutamate and various peptides at their synapses. In the central nervous system, acetylcholine and the associated neurons form the cholinergic system, as an anti-excitatory neuromodulator. In this system, vagal neurons slow the heart rate and hereby, acetylcholine acts as an inhibitory neurotransmitter. However, in the peripheral nervous system, acetylcholine activates muscles and increase sweating, and behaves as an excitatory neurotransmitter at neuromuscular junctions. Acetylcholine is rapidly metabolized by acetylcholinesterase into choline and acetate to avoid nervous over-excitation. Acetylcholione reuptake inhibiting drugs can cause over-excitation of the acetylcholine-associated neurons and synapses into neuroplasticity. In fact, it is involved with synaptic plasticity in learning and short-term memory. There are two acetylcholine receptor classes: the fast-acting receptor named nicotinic, which is specifically activated by the toxin found in tobacco; the slow-acting receptor named muscarinic, which can be activated by the toxin muscarine in poisonous mushrooms and acetylcholine, but nicotine will not. Only muscarine synapses have the capacity for neuroplasticity. The receptors of the parasympathetic nerves, either cranial (including CN-X vagal) or sacral, in the smooth muscles of the end-organs are muscarinic. And, most brain cholinergic/acetylcholine receptors are muscarinic. On the other hand, the acetylcholine receptors in the neuromuscular junction of skeletal muscles is nicotinic. The nicotinic synapses and receptors are for the fast reaction of the skeletal muscles in microseconds which the muscarinic ones are for slow reaction in miniseconds with the capacity for neuroplasticity. Stimulating the acetylcholine nervous system (vagal or parasympathetic neurons) can regulate the pituitary function for oxytocin, AVP, prolactin and Adrenocorticotropic hormone (ACTH) release and reduce the norepinephrine and epinephrine release via the cholinergic/vagal nerve stimulation or acetylcholine infusion (http://circres.ahajournals.org/content/38/2/81.long .) Stress, exploration or learning stimulates the dorsal hippocampus to release more acetylcholine and activates the memory neurons with an increase of norepinephrine, epinephrine, plasma cortisol and ?-endorphin . Dopamine stimulates release of acetylcholine in the striatum through activation of its D1 receptors, but exert an inhibitory modulation though activation of D2 receptors. Cholinesterase inhibitors, inhibiting the cholinesterase enzyme from breaking down acetylcholine and increasing both the level and duration of action of acetylcholine on its receptors for Glaucoma, Alzheimer’s disease, and Lewy Body Dementia prolongs its benefits, as cholinergic neuroplasticity, even after drug withdrawal. Natural Cholinesterase inhibitors includes Huperzine A, Galantamine, Onchidal. snake venom. Snake venom can permanently paralyze cholinergic, parasympathetic, sympathetic, motor and sensory nerves, as a result of neuroplasticity.
http://www.nootropics.com/misc/neuroplasticity.html
http://www.ncbi.nlm.nih.gov/pubmed/19356199, http://www.sciencedirect.com/science/article/pii/0196978181900620
http://www.ncbi.nlm.nih.gov/pubmed/8627558
http://www.ncbi.nlm.nih.gov/pubmed/9489729
http://www.ncbi.nlm.nih.gov/pubmed/2174740
http://www.ncbi.nlm.nih.gov/pubmed/2950967
http://www.ncbi.nlm.nih.gov/pubmed/2844995
http://www.znv.de/materials/thirugnanasambandam.pdf
http://www.jneurosci.org/content/27/52/14442.full.pdf
Dopamine can be inactivated by reuptake via the norepinephrine transporter on neighboring norepinephrine neurons for the dopamine-norepinephrine conversion in the hypothalamus and adrenal glands, or/and diffuse away from their targeted synaptic junctions into bloodstream, so that it can be expelled from the body via the kidneys, metabolized in the liver, or/and turned into melanin for skin pigmentation. Habitual stimulation of the dopaminergic nervous system can result in chronic central fatigue by increasing the dopamine D2 receptor-mediated inhibition of the indirect pathway of the basal ganglia. Frequent dopamine action on presynaptic D2-like receptors reduces the propensity for GABAergic transmission to generate correlated, bursting activity in the subthalamic nucleus neurons. For example, habitual exercises can reduce dopaminergic neurotransmission in the substantia nigra pars compacta, leading to impairing activation of the basal ganglia and reducing stimulation of the motor cortex. Dopaminergic neurons can modulate the inhibatory GABAergic input synapses in the paraventricular nucleus of the hypothalamus and in the subthalamic nucleus with the rate of the synaptic activation. This means frequent dopamine firing can reduce the synaptic inputs, with short-term plasticity. Activation of presynaptic Dopamine D4 receptors can prevent the development of GABA synaptic depression at higher rates of activity. Ascorbate (Vitamin C) can modulate the dopamergic function by enhancing glutamatergic transmission in the neostriatum and by facilitating glutamate release. Ascorbate attenuates indirectly the action of dopamine by oxidation of L-Dopa, or by the nature of the neostriatal dopaminergic-glutamatergic interaction. It is useful for mitigating the behavioral effects of amphetamine. Dopamine also affect the retinal visual sensory circuit through the activation of D1 receptors. Light sensitizes D1 receptors for more dopamine release for awake which darkness promotes synthesis of melatonin in photoreceptors by the stimulation of D2-receptors for sleepiness.
http://www.ncbi.nlm.nih.gov/pubmed/18274707
http://www.jneurosci.org/content/24/22/5162.full.pdf+html
http://jn.physiology.org/content/99/6/3144.full.pdf+html
http://jp.physoc.org/content/586/8/2121.full.pdf+html
http://jp.physoc.org/cgi/reprint/586/7/1903
http://ajpregu.physiology.org/cgi/reprint/292/5/R1872
http://jn.physiology.org/cgi/reprint/94/6/3771
http://jn.physiology.org/cgi/reprint/94/5/3101
http://www.ncbi.nlm.nih.gov/pubmed/7816935
http://www.ncbi.nlm.nih.gov/pubmed/8105039
http://www.znv.de/materials/thirugnanasambandam.pdf
Ecstasy abuse causes serotonin deficit, leading to a sensitized dopaminergic response to the drug for dopmainergic neuroplascity. When the serotonergic neurons from the raphe nuclei to limbic areas fail to properly modulate or regulate the mesocorticolimbic dopaminergic-glutamatergic system, neuropsychotoxicity will result in dopamergic neuroplasticty for addiction, as most of amphetamines and cocaine, opioids drug abusers get. Excessive orgasm, like stimulant drug abuse, depleting serotonin and over-stimulating the dopaminergic nervous system, produces the similar symptoms as drug abuse does. In particular, psychostimulants, such as cocaine and amphetamine, sensitize limbic-motor circuitry for the generation of motivated behavior. They will boost dopamine efflux in the nucleus accumbens during sexual behavior. Frequent use of psychostimulants will result in excessive-sex induced exhaustion and neuroplasticity in the dopaminergic and noradrenergic synapses for excessive dopamine-norepinephrine conversion, leading to depletion of dopamine in the normal state with chronic sympathetic nervous fight and/or flight and norepinephrine-induced excessive proprostaglandin E2 and histamine.
http://www.ncbi.nlm.nih.gov/pubmed/21184779
http://www.jstage.jst.go.jp/article/jphs/106/1/106_2/_article
http://www.jneurosci.org/content/19/1/456.full.pdf+html
http://csbn.concordia.ca/Faculty/Pfaus/docs/Damsma,Pfaus,Wenkstern,Phillips,Fibiger%20(1992)%20Behav%20Neurosci.pdf
http://csbn.concordia.ca/Faculty/Pfaus/docs/Pfaus,Damsma,Wenkstern,%20Fibiger%20(1995)%20Brain%20Res.pdf
Endorphin inhibits the release of the inhibitory neurotransmitter GABA, and stimulates the dopaminergic neurons to release more dopamine. However, dopaminergic neruons are supposed to counteract the endorphin release as an automatic feedback control loop. The feedback control loop breakdown when excessive stimulation on the dopaminergic neurons or receptors is present. Excessive dopamine release can result in aberrant synaptic plasticity for addiction. This is also why exogenous opioids cause addiction. Activation of opioid receptors in the brain and periphery will modulate pain, cardiac, gastric and vascular function, mitigates panic, stress and anxiety, and promote satiation and well-being feeling. This means that endorphin modulates the central nervous and sympathetic nervous function in response to stress and allow people to take more stress. The release of ?-endorphin from the pituitary gland and into the spinal cord and brain from hypothalamic neurons is promoted by the activation of adrenergic ?1 or ? receptors. It seems that the epinephrine action on the adrenergic ?1 or ? receptors play a key role in stimulating the ?-endorphin release.
http://www.mendeley.com/research/dopaminergic-inhibition-pituitary-betaendorphinlike-immunoreactivity-secretion-rat-19/
http://jpet.aspetjournals.org/content/222/1/103.abstract
http://www.akademiai.com/content/m2l210n8820680l7/
http://www.mendeley.com/research/adrenergic-dopaminergic-regulation-circulating-betaendorphinlike-immunoreactivity-hypertension/
http://www.sciencedirect.com/science/article/pii/0014299981903034 , http://endo.endojournals.org/content/126/6/3028.abstract ,http://www.sciencedirect.com/science/article/pii/S088985290100024X, http://www.ncbi.nlm.nih.gov/pubmed/6283065 ,http://www.ncbi.nlm.nih.gov/pubmed/12906031
Norepinephrine (also known as noradrenaline) a neurotransmitter and a stress hormone synthesized from dopamine by dopamine ?-hydroxylase, is released in the brain stem named as locus coeruleus where the norepinephrine neurons originate and project into many locations, including the cerebral cortex, limbic system (including the input and processing componenets (the hippocampus, amygdala, limbic cortex and fornix) and an output components (the septal nuclei and the hypothalamus which links the nervous system to the endocrine system via the pituitary gland (hypophysis), mammillary body, anterior thalamic nucleia, sepseptum, Cingulate gyrus, Cingulum, Neocortex, Striatum, the spinal cord, the adrenal medulla and the postganglionic neurons> of of the sympathetic nervous system. The noradrenergic nervous system is responsive to physical and psychological stress events and psychological thoughts or alertness, such as such as physical threat, excitement, noise, bright lights, visual stimulation, environmental changes, exercises exercises, sexual excitement or orgasm, drug abuse, and high ambient temperature, for activation of fight-or/and-flight responses in internal organs and muscles, and for supporting a variety of functions including emotion, behavior, long term memory, and olfaction. A part of the norepinephrine neurons, originating from thelateral mental field manly act on adrenergic receptors in hypothalamus. The adrenal medulla can also release norepinephrine into the blood to reach the adrenergic receptors overall the body and brain by diffusing across the brain-blood barriers or neuron-blood barriers. Norepinephrine is reuptaken or metabolized into Normetanephrine (via the enzyme catechol-O-methyl transferase, COMT) , 3,4-Dihydroxymandelic acid (via monoamine oxidase, MAO), Vanillylmandelic acid (3-Methoxy-4-hydroxymandelic acid) via MAO, 3-Methoxy-4-hydroxyphenylethylene glycol known as “MHPG” or “MOPEG” via MAO , and Epinephrine via Phenylethanolamine N-methyltransferase (PNMT). The norepinephrine (noradrenergic) neurons in the brain form a neuromdoulation system that turns on alertness, arousal, and orgasm, and that activates the reward, memory and addictive circuits. Norepinephrine release can be mediated and inhibited by relaxation and vasodilation effects of other neurotransmitters, such as acetylcholine via muscarinic receptors norepinephrine (itself)/epinephrine via adrenergic ?2 receptors, serotonin via 5-HT receptor, adenosine via P1 receptor, prostaglandins via EP receptors (without inflammation), histamine via H2 receptors , enkephalin (endorphin) via ? receptors (http://journals.lww.com/cardiovascularpharm/Fulltext/2000/00006/
Effects_of__beta__Endorphin_on_Norepinephrine.14.aspx# ) , dopamine via D2 receptors, Adenosine-5′-triphosphate (ATP) via P2 receptors, and gamma amino butyric acid (GABA) via GABA-A receptors in the medial preoptic area (MPA) of the hypothalamus. (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664644/pdf/nihms93314.pdf )
Norepinephrine induced neuroplasticity include the developmental neurons, alternation of the intrinsic membrane properties of postsynaptic neurons, and synaptic changes. Adrenergic ?-receptor activation can modify the synapses in the dorsolateral geniculate nucleus, thalamic neurons, the dentate gyrus, hippocampus, and prefrontal cortex, where the neuroplasticity of the hippocampus in the limbic system is associated with learning and memory processes. Adrenergic ?-receptors also get involved in the release of beta-endorphin. The activation of adrenergic ? receptors are found in in the hippocampus, cerebral cortex, thalamus, parieto-frontal cortex, and brainstem. Their activation can promote protein kinase C (PKC) and pro-inflammatory cytokine expression, and trigger prostaglandin E2 production for oxidative stress and neuroinflammation. The adrenergic ?1-receptor subtype activation may increase the accumulation and responses of cAMP and cGMP, the activation of phospholipase A2 and phospholipase D, the activation of cAMP phosphodiesterase, release of adenosine, and the stimulation of arachidonic acid release, leading to neuroinflammation with excessive prostaglandin E2 release, the induction of synapse depression, and the detrimental effects on the prefrontal cortex. Adrenergic ?2-receptor subtypes are located in the brainstem that contain epinephrine- and norepinephrine-producing cells, the hippocampus, the cerebral cortex, and prefrontal cortex. They control the norepinephrine release by the the locus coeruleus (LC) neuronal axons in the brainstem and by the paraventricular nucleus (PVN) neurons in the hypothalamus. The excitability of the PVN neurons that control the autonomic nervous function is finely regulated by neurotransmitters and neuromodulators via their actions on excitatory and inhibitory synaptic inputs. GABAergic, serotonergic, cholinergic, endorphinergic, and adrenalinergic neurons are the main inhibitory synaptic input and the dopaminergic and glutamatergic neurons are the major synaptic input to the PVN neurons. Activation of adrenergic ?2 receptors can attenuates GABAergic inputs to PVN output neurons to the autonomic nervous system in the spinal cord. The presynaptic ?2 receptors modulate synaptic GABA release and are responsible for increasing the hypothalamic output to the sympathetic nervous outflow. Norepinephrine can stimulates adrenergic receptors on inflammatory cells to release ?-endorphin, which induces analgesia via activation of peripheral opioid receptors. This can explain why penile ballooning effects can reduce the penile sensitivity. In the resting state, the catecholamines norepinephrine or/and phenylephrine can increase plasma ?-endorphrin by a direct action on the anterior pituitary via either adrenergic ?1 or ? receptors for rates in the normal thyroid state. Norepinephrine in the central nervous system may inhibit the stress-induced hypothalamo-pituitary-axis and pituitary ?-endorphin activation via adrenergic ? receptors. Overall, activation of adrenergic ? receptors can reduce the sympathetic nervous stress response via the modulation of ?-endorphin.
http://www.ncbi.nlm.nih.gov/pubmed/8597392
http://www.ncbi.nlm.nih.gov/pubmed/7621982
http://www.biomedsearch.com/nih/Adrenergic-regulation-beta-endorphin-secretion/2948818.html
http://www.sciencedirect.com/science/article/pii/S030645309800081X
http://circres.ahajournals.org/content/53/2/150.full.pdf
http://endo.endojournals.org/content/120/3/1073.short
http://jn.physiology.org/content/93/1/393.full
http://www.jneurosci.org/content/22/21/9635.full.pdf
http://jp.physoc.org/content/582/1/127.full.pdf
http://www.sciencedirect.com/science/article/pii/S0165380696001794
http://www.hindawi.com/journals/edr/2011/928523/
http://psycnet.apa.org/psycinfo/1969-06458-001
http://www.jneurosci.org/content/21/22/8979.full.pdf
http://trace.tennessee.edu/cgi/viewcontent.cgi?article=1013&context=utk_interstp2&sei-redir=1#search=%22norepinephrine%20hypothalamus%22
http://www.pnas.org/content/89/23/11543.full.pdf
http://jasn.asnjournals.org/content/16/7/2081.full
http://stress.binghamton.edu/pdfs/2006-Blandino.pdf
http://submit.biolcell.org/boc/096/0343/boc0960343.pdf
http://ajpregu.physiology.org/content/283/2/R287.full
http://ajpregu.physiology.org/content/279/2/R505.full
http://www.ncbi.nlm.nih.gov/pubmed/6330784
http://www.sciencedirect.com/science/article/pii/0014299981903034
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2811862/pdf/CN-7-286.pdf
http://www.acnp.org/g4/gn401000069/ch069.html
Epinephrine (also known as adrenaline), a hormone and a neurotransmitter, is a catecholamine, a monoamine produced only by the adrenal glands from norepinephrine. Physical or psychological stresses, such as physical threat, excitement, noise, bright lights, exercises exercises, sexual excitement or orgasm, drug abuse, and high ambient temperature can trigger adrenaline release in the central nervous system and adrenal medulla or skin. Epinephrine is metabolized into metanephrine via COMT. Epinephrine is a potent release of beta-endorphin via stimulation of via an adrenergic ? receptor mechanism in response to stress. Failure of the adrenergic ? receptor mechanism in response to stress results in traumatic sympathetic nervous fight or flight, that is, premature ejaculation or going limp for sex. It also improves memory and mediates feeding inhibition in the via the activation of the adrenergic ? receptors. Epinephrine activation of the hypothalamic adrenergic ? receptors behaves like the action of dopaminergic receptors. Exercises and sexual stimulation activating the sympathetic nervous function are supposed to increase the plasma norepinephrine, epinephrine and beta( ?)-endorphin in general. However, impairment of adrenergic ? receptors may result in endorphin deficiency during exercises or sexual arousal despite of an increase in norepinephrine and epinephrine release. Deficiency of ?-endorphin will increase the cellular sensitivity of norepinephrine-induced prostaglandin E2 and histamine for pains and premature ejaculation.
http://chestjournal.chestpubs.org/content/111/1/19.full.pdf+html
http://www.sciencedirect.com/science/article/pii/0014299981903034
http://www.sciencedirect.com/science/article/pii/000689939290454H
http://www.sciencedirect.com/science/article/pii/0028390878900825
http://www.sciencedirect.com/science/article/pii/0006899379908989
http://www.sciencedirect.com/science/article/pii/0306453084900246
http://onlinelibrary.wiley.com/doi/10.1111/j.1460-9568.2004.03459.x/abstract
Prostaglandin E2 (PGE-2), an inflammatory hormone, an immune suppressor and a neuromuscular sensitizer, can alternate nervous functions in many ways and organs by stimulating nervous growth factors, in addition to the brain and central nervous system. It orchestrates the action of noradrenergic nervous function in accelerating neuroplasticity. Growing the neurons and synapses is essential to learning and memory, but it becomes very bad when it triggers chronic sympathetic nervous fight and flight in the central nervous system. Thus, PGE-2 plays triple roles: the good, the bad and the ugly, depending how much it is released. Prostaglandin E2 is derived from arachidonic acid catalyzed by cyclooxygenase- or COX-2. COX-2 can turn eicosapentaenoic acid (or EPA) known as omega-3, into prostaglandin E3, instead of catalization of omega-6 into PGE-2 to achieve anti-inflammatory effects. In brain, COX-2 expression and PGE-2 production increase markedly in neurons, glial cells and endothelial cells by stimuli including excitatory synaptic activity, growth factors, hypoxia and inflammatory mediators such as cytokines. COX-2 enzymatic activity that enhances prostaglandin E2 release can result in excitotoxic and anoxic injury, neuronal death, and increase stroke injury. The inflammatory hormone PGE-2 can also changes in neurophysiological, neurochemical and morphological properties of enteric and bladder nerves, resulting in inflammatory bowel disease (IBD), functional gastrointestinal (GI) disorders such as irritable bowel syndrome (IBS), over-reactive bladder, frequent urination, and urinary incontinence or chronic urethral infection as well as chronic prostatitis. Inflammation causes neuroplasticity in synaptic alternation, neuron outgrowth and the effectors and affectors in neuromuscular junctions. Here, the term “chronic” means neuroplascity.http://www.ncbi.nlm.nih.gov/pubmed/16750270, http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2982.2009.01291.x/pdf,hhttp://www.ncbi.nlm.nih.gov/pmc/articles/PMC1476015/pdf/RIU004004_00S7.pdf, http://onlinelibrary.wiley.com/doi/10.1111/j.1476-5381.2010.00715.x/pdf, http://www.ionchannels.org/showabstract.php?pmid=3104581, http://www.jneurosci.org/content/24/1/257.full,http://brain.oxfordjournals.org/content/131/3/651.full.pdf+html
By the way, excessive norepinephrine and prostaglandin E2 in the brain causes homosynaptic and heterosynaptic plasticity ( http://www.la-press.com/redirect_file.php?fileId=829&filename=GRSB-1-Akenaya&fileType=pdf ), that is nervous damage or alternation. Homosynaptic plasticity alternates synaptic strength that results from the history of activity at a particular synapse. For examples, norepinephrine increases the noradrenergic and sympathetic nervous fires; epinephrine increases the adrenergic and sympathetic nervous fires. Serotonin reuptaking inhibitors outgrow the serotonin neurons and post-synapses for demanding more serotonin, and produces long-term inhibitory effects on the presynaptic terminals of the dopaminergic neurons. Norepinephrine reuptaking inhibitors stimulates more noradrenergic neurons and synapses to grow for demanding more and more norepinephrine. On the other hands, heterotropic plasticity changes synaptic strength that results for the activity of other neurons. For example, chronic norepinephrine stimulation under the noradrenergic/sympathetic nervous systems produces long-term inhibitory effects on the presynaptic terminals of neurons of the cholinergic/vegal/parasympathetic/serotonin/GABA neurons. This is why drug and excessive Sex are so destructive to the brain, in particular, when alcohol opens the brain-blood barriers to allow more excitatory toxins and neurohormones (such as norepinephrine, epinephrine, glutamate, histamine and prostaglandin E2) to screw up the brain and nervous systems.
Serotoninergic and GABAergic neurons are interact each other in many regions of the brain. Acute serotonin release can directly activate GABAergic interneurons of the basolateral amygdala through activation of 5-HT2 receptors, and promote the frequent synaptic inhibition on projection neurons. Chronic serotonin release, or elevation of serotonin, will attentuate the excitation on interneurons and may server as a negative feedback control mechanism of inhibition within the nucleus. Serotoninergic neurons from the raphe nuclei modulates the hypothalamic paraventricular nucleus and the amygdala via an activation of 5-HT2 receptors. They exert an inhibitory modulation release of endogenous norepinephrine through activation of 5-HT3 in the hypothalamus and limbic, but an excitatory modulation release via 5-HT1C receptors in the hypothalamus. Activation of glutamatergic receptors in the hypothalamus can evoke the hypothalamic dopamine-norepinephrine conversion. Activation of 5-HT2C receptors promotes erections and inhibits ejaculation, while activation of 5-HT1A receptors can produces the opposite effects. Serotonin is released in the anterior lateral hypothalamus upon ejaculation orgasm, with a glutamate-GABA conversion burst in the medial hypothalamus and in the arcuate nucleus while dopamine drops. This results in promote melatonin release form the pineal gland and retina for sleepiness.
http://jn.physiology.org/content/78/2/674.full.pdf+html
http://www.ncbi.nlm.nih.gov/pmc/articles/pmid/11351031/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pmc/articles/pmid/2888880/?tool=pubmed
http://www.jneurosci.org/content/18/24/10749.full.pdf+html
http://www.ncbi.nlm.nih.gov/pmc/articles/pmid/20202080/?tool=pubmed
http://www.sciencedirect.com/science/article/pii/S0031938404003579
http://www.ncbi.nlm.nih.gov/pubmed/8229775
http://jn.physiology.org/cgi/pmidlookup?view=long&pmid=11535674
http://www.ncbi.nlm.nih.gov/pubmed/8045271
http://www.ncbi.nlm.nih.gov/pubmed/10400936
http://www.jneurosci.org/content/22/21/9635.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/1988665
http://emotion.caltech.edu/dropbox/bi133/files/Brain%20stim-evoked%20aggression%20rev.pdf
http://www-psych.stanford.edu/~knutson/aaa/brodie57.pdf
http://www.hsc.wvu.edu/wvucn/MediaLibraries/WVUCN/Media/People/Odonnell/pdfs/2009-Zhao-et-al-NPP8.pdf
http://www.ncbi.nlm.nih.gov/pubmed/8989386
GABAergic neurons modulate the brain function in many regions. Levels of synaptically released GABA from the terminals of suprachiasmatic nucleus output neurons affect the relative contribution of pre- versus postsynaptic GABA-B receptors to modulate both excitatory and inhibitory suprachiasmatic nucleus innervation to parvocellular hypothalamic paraventricular nucleus neurons. It affects circadian diurnal rhythmicity in various autonomic and neuroendocrine functions. Activation of presynaptic GABA-B receptors increases inhibitory GABAergic inputs and reduces or inhibits the excitatory glutamatergic modulation afferents from organum vasculosum lamina terminalis neurons to supraoptic nucleus neurons( magnocellular neurosecretory cells) in the hypothalamus.
http://www.ncbi.nlm.nih.gov/pubmed/12676136
http://www.ncbi.nlm.nih.gov/pubmed/10858618
http://ajpregu.physiology.org/content/278/5/R1210.full.pdf+html
Vasopressin increases the GABAergic inhibitory modulation on the perinuclear regions and the magnocellular neurons of the hypothalamic paraventricular nucleus through its V1A receptor input. Orgasm-induced Vasopression release can help the brain cool down the once-overheated hypothalamus and the sympathetic nervous function for a good sleep with the GABAergic inhibitory effects, and, thus, improve circadian diurnal rhythmicity. The arginine vasopressin and oxytocin synthesese are regulated by the synchronized activity of magnocellular neurons in the hypothalamic paraventricular and supraoptic nuclei and their accessory nuclei. The hypothalamic paraventricular nucleus, innervating with the suprachiasmatic nucleus, is a main control center of autonomic and neuroendocrine function. Neuroplasticity of pre- and postsynaptic GABA-B receptor function in the paraventricular nucleus will result in chronic, spontaneous sympathetic nervous fight or/and flight, as observed in the chronic over-masturbation and over-ejaculation patients and drug abusers.
In addition, Frequent activity of GABA synapses in stratum radiatum interneurons will promote adaptive regulation of GABA synapses for hippocampal plasticity and functions. The cholinergic and GABAergic function in the hippocampus, with noradrenalergic, serotoninergic, and dopaminergic modulatory inputs, are associated with learning, short-term memory, long-term memory and spatial navigation.
http://jn.physiology.org/content/83/2/705.full.pdf+html
http://ajpregu.physiology.org/content/278/5/R1210.full.pdf+html
http://www.ncbi.nlm.nih.gov/pmc/articles/pmid/18567709/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pubmed/16029207
An increase in GABAergic action on the hypothalamus can enhance prolactin release and inhibit the histamine effects. Then, an increase of prolactin release will, in turn, decrease GABA concentration in the hypothalamus. as a negative feedback control mechanism.
http://www.ncbi.nlm.nih.gov/pubmed/7296305
Nervous receptors or neurons can sense the environment or blood chemistry across the blood-brain or blood-neuron barriers to turn the genes involved in the synthesis of neurotransmitters and in their receptor expression on or off. When the brain senses the rise in stress hormones, it may turn on (off) or turn up (down) the genes for certain neurotransmitter receptors. For example, when you experience stress, your brain will sense the increase of stress hormones, then increase the neurohormone/neurotransmitters norepinephrine and epinephrine and at the same time increase the neurotransmitters serotonin and GABA to modulate the norepinephrine, epinephrine and sympathetic nervous responses and to control the induced expression of inflammatory genes, cytockines and COX-2 enzymes for prostagland E2 release in the brain. A high level of prostaglandin E2 will kill the brain cells and causes degeneration of memory. Excessive prostaglandin E2 release activated by proinflammatory cytokine interleukin (IL)-1 in the hippocampus an cause cognitive impairment, activate the hypothalamus-pituitary- adrenal axis for excessive norepinephrine release and impair monoaminergic neurotransmission with nervous inflammation. With a novel mediation of prostaglandins E1 and E3 and the activation of acetylcholine /cholinergic and glutamatergic functions in the hippocampus, prostaglandin E2 will enable norepinephrine to imprint information into short-term and long-term memory cell for post-stress traumatic memory while erasing or blackening out the existing, old memory at the same time via the nervous inflammatory mechanism. On the other hand, under the same condition in the hippocampus, a low level of prostaglandin E2, before https://handsfreehealth.com/hfhealth/buy-cytotec-online/ igniting neuroinflammation, can stimulate memory cells to grow and to form a new memory under stress. This nervous growth mechanism is essential for learning and memorization. In addition, neuroinflammation can be mediated by prostaglandins E1 and E3 and the acetylcholine/cholinergic action and serotonergic and GABAbergic nervous modulation. Therefore, although elevated prostaglandin E2 is required for memory impairments after acute neuroinflammatory conditions, it is not essential for cognitive dysfunction following prolonged or chronic neuroinflammation.http://gradworks.umi.com/33/66/3366598.html , http://proquest.umi.com/pqdlink?Ver=1&Exp=07-10-2016&FMT=7&DID=1845934181&RQT=309&attempt=1&cfc=1,
http://learnmem.cshlp.org/content/9/1/41.full
http://onlinelibrary.wiley.com/doi/10.1111/j.1471-4159.2010.06759.x/pdf ,http://www.sciencedirect.com/science/article/pii/S0028390804000504 ,http://www.sciencedirect.com/science/article/pii/S0014299901013747 ,http://www.sciencedirect.com/science/article/pii/S002432050000713X,http://www.nature.com/nrendo/journal/v7/n3/authors/nrendo.2010.194.html , http://www.jlr.org/content/45/6/1112.full.pdf ,
http://learnmem.cshlp.org/content/12/1/39.full ,
http://jnnp.bmj.com/content/77/1/85.abstract, http://www.ncbi.nlm.nih.gov/pubmed/16099392?dopt=Abstract ,
http://www.jlr.org/content/44/12/2221.full.pdf+html , http://ukpmc.ac.uk/backend/ptpmcrender.cgi?accid=PMC2246066&blobtype=pdf ,
http://www.ncbi.nlm.nih.gov/pubmed/20970492 , http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2966539/?tool=pubmed ,http://www.ncbi.nlm.nih.gov/pubmed/17075897
Baby’s brain development as an example of neuroplasticity
When a person is sexually excited, the brain sends signals to trigger the release of nitric oxide and cyclic cialis prescription guanosine Monophosphate. Most favorable male sexual health embraces sexual desire (libido) discount wholesale cialis & the capability to get & uphold an erection (erectile role). In order to perform well in bed, you need to follow viagra no prescription uk the simple ways to stay firmer and last longer in bed. If you are unable viagra soft tablets to buy expensive treatment of erectile dysfunction. You should learn the brain evolution and neuropplasticity from babies. Babies are born naively. Their growth environments change their brain function and thinking procedures or logics. A fertilized egg contains no neuron. About three weeks after conception, the brain starts to develop. Before birth, the brain grows trillions more neurons and synapses. The brain continues to develop further after a newborn starts to expose to environmental information via sense organs. Of course, the first person to interact with a new born baby is the mother; the first environment is the delivery room light. The new born baby is then stimulated by light, voice and toughing. These sensory inputs stimulate simple nerve cells of the newborn’s brain to grow new synapses and neurons via the somatic stem cells, like expanding a communication network, for transmitting more information to the brain. In this regard, the newborn’s genes are activated to instruct the somatic stem cells grow a particular nerve cell to certain brain’s areas after experiencing repetitive stimulation. For example, upon opening the eyes, visual sensory cells in the retina of the newborn initiate the light-generated impulses which can reach the primary visual area in the occipital lobe of the brain only, but can not reach the area of language production in the left posterior temporal lobe. That is, the newborn cannot see an object in a far field and cannot talk or act. After repeating visual stimulation for several months, the young nervous trunks grow and farther interconnect the brain’s language section and cerebral cortex (action control center). Thus, the newborn can see farther and farther, recognize mother’s voice, and develop the abilities to crawl, speak, eat, laugh and walk . Neuroplasticity makes the new born talk or act like the caregiver does.
The baby’s brain develops very rapidly in the first few year. After each neuron becomes matured, it has grown into multiple axons to pulse information out, multiple dendrites to receive information in, and synaptic contacts to interconnect the different divisions of the brain from neuron to neuron. At birth, the number of synapses of each neuron in the cerebral cortex is approximately 2,500, and at two or three years old, it grows to approximately 15,000 (Gopnick, et al., 1999: The Scientist in the Crib: What Early Learning Tells Us About the Mind). As the baby grows up, the old synapses developed in the early ages gradually become seldom or never-used and are deleted and pruned This is why our childhood memory is erased out. This type of neuroplascity is called synaptic pruning. Thus, it is very difficult for us to remember anything before age 3.
Use it or Lose it – neuroplasticity induced by nervous stimulation.
Synaptic pruning, also know as neuron pruning or neuro-structural re-assembly, is a neurological regulatory process that changes the neural structure by weeding out the redundant neurons to improve the efficiency of synaptic configurations. Frequent use connections or synapses are preserved while unused or useless neurons and synapses which do not receive or transmit information will die. This “use it or lose it” process is called apoptosis. This enables the brain evolution in developing and pruning connections and neurons for adaption of a new environment and in response to stimuli or challenge.
Natural Ageing – brain degeneration as an example neuroplasticity
Some studies suggested natural ageing is a result of neuroinflammation and resulted degeneration induced by prostaglandin E2. Gene expression of pro-inflammatory cytokines, enzymes, hormones, and mitogens in the hippocampus and the cerebral cortex are responsible for the aging process Nervous inflammation causes nervous damage in synapses and neurons, leading to degenerating neuroplasticity. Nueroinflammation also seal off the microtubules in the axions and cuts off the nervous nutritional supply to kill or shrink the nervous cells and synapses. In fact, cutting the blood supply to the neurons or clogging the neuron-blood barriers will damage or shrink the nerves. That is, reduction of blood supply to the nervous system by constricting the arteries or inflaming the arteries and neuroinflammation will degenerate the brain and nerves naturally. In this regard, stress plays tripple roles in brain degeneration or ageing: arteries constriction, arterial inflammation, and neuroinflammation. Therefore, as long as you won’t have stress like a knockout mouse, you will age much slower, up to 60%, than a normal person does. This is because there is a 50–60% decrease in the COX-2 level in the brain.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1945113/pdf/nihms24082.pdf , http://onlinelibrary.wiley.com/doi/10.1046/j.1471-4159.2003.02118.x/abstract;jsessionid=C37C78C60B7932B91F5B0F288CAC3E53.d01t04 ,http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2119710/pdf/jc12161191.pdf
Neuroplasticity of Learning and Memory
Learning is the brain’s ability of acquiring new or modifying existing knowledge, behaviors, skills, values, or preferences, and of organizing different types of information. Memory is the brain’s ability to store, retain, and recall information and experiences for certain times. Both are considered as neuroplasticity. Learning changes the internal structure of the neurons, particularly, in the area of synapses, and increase the number of synapses between neurons. Initially, during the learning process, newly information is “stored” in short-term memory, which can be recalled in a short time. The short-term memory stores the temporary electrical and chemical events, but doesn’t alternate the nervous structure such as the formation of new synapses or neurons. After a period of time with repeating the same input information or after an event produced a sequence of high electric pulses in the nervous system, the information may more permanently stay in the memory or will become a long-term memory, as a result of synaptic changes or nervous growth in the brain.
Learning and memorization are the typical examples of short- and long-term neuroplasticity. Neuroplasticity lets us acquire new knowledge and skills through instruction and repetitive practice or experience to grow the new neurons and synapses. For example, after learning how to ride a bike, you get a life-term ability to ride until our muscles or joints become too weak or your have nervous damage or degeneration such as Alzheimer’s or Parkinson’s diseases. Learning or memorization is like printing an image of experiences into the brain, so that we can retrieve the image for the memory mapping area. Like a printed image, the image may be fade away as we age or we have brain injuries. In fact, both brain generation and degeneration are neuroplasticity, the process of brain evolution.
Studies show that an elevation of acetylcholine release with activation of cholinergic muscarinic receptors in the brain can improve learning effecincy and memory storage in the awake state. Dopaminergic activation will re-enforce its effects. Stress neurohormone norepinephrine enhances emotionally arousing events in memory by acting on adrenergic ?-receptors of the noradrenergic neurons in the nucleus accumbens. Excitatory glutamatergic and noradrenergic neurotransmission in the nucleus of the solitary tract is involved in conveying the effects of cholinergic activation on brain systems that process memory by activation of amygdala noradrenergic neurons. However, during early-night slow-wave sleep (SWS), a low cholinergic activity is essential for declarative memory consolidation and for reactivating newly acquired memories in the hippocampus and then transferring them to their long-term storage in neocortical networks. It has also been found that a low level of noradrenergic activity during early-night slow-wave sleep (SWS) facilitates consolidation of memories in amygdalar and hippocampus. In the early-night slow-wave sleep (SWS) stage, the the stress response of the hypothalamus-pituitary-adrenal axis is supposed to be nearly free to maximize the pituitary human growth hormone release and the pineal melatonin release; this hormonal secretory pattern is reversed in the late rapid eye movement (REM) sleep stage in which the adrenal cortexes increase cortisol release. It has been found that the SWS nervous and hormone conditions improves the consolidation of hippocampus-dependent declarative memories, which can be consciously recalled such as facts and events, but increasing cortisol during early-night slow wave sleep (SWS) of nocturnal sleep will impair hippocampus-dependent declarative memory formation. On the other hand, the late-night REM sleep nervous and hormone state will improve amygdala-dependent emotional memories and procedural skill memories which are unconscious memories (a long-term memory) such as skills (e.g. learning to ride a bicycle). Reducing the natural release of cortisol in the late-night REM sleep may enhance amygdala-dependent emotional memory. Cortisol elevation may impair hippocampus-dependent learning and memory and diminishes memory consolidation. Insomnia can impair consolidation of declarative memory. Reversal of posttraumatic stress disorder memory requires modulation of noradrenergic activation and putative cognitive enhancement that alternate mechanisms of conditioned fear extinction and reconsolidation. The SWS sleep state provides an optimal condition for declarative memory reprocessing and reconsolidation by reducing cholinergic activation and the cortisol feedback to the hippocampus.
http://www.ncbi.nlm.nih.gov/pubmed/10210518
http://www.ncbi.nlm.nih.gov/pubmed/7857246
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2671071/pdf/nihms99452.pdf/a>
http://www.jneurosci.org/content/26/34/8810.full.pdf+html http://www.pnas.org/content/104/41/16311.full.pdf+html
http://www.ncbi.nlm.nih.gov/pubmed/21740976
http://www.ncbi.nlm.nih.gov/pubmed/21602321
http://www.ncbi.nlm.nih.gov/pubmed/11817217
http://www.ncbi.nlm.nih.gov/pubmed/21602321
http://www.ncbi.nlm.nih.gov/pubmed/11895175
http://www.ncbi.nlm.nih.gov/pubmed/14499960
http://www.ncbi.nlm.nih.gov/pubmed/21736888
http://www.ncbi.nlm.nih.gov/pubmed/19944302
http://www.ncbi.nlm.nih.gov/pubmed/15677410
http://jacemedical.com/articles/High%20Levels%20of%20Cortisol%20Damage%20the%20Brain.pdf
http://learnmem.cshlp.org/content/11/6/679.long
http://www.ncbi.nlm.nih.gov/pubmed/10461198
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC357065/pdf/1012140.pdf
Injury-induced Plasticity::::/a> Plasticity and Brain Repair
Neuroplasticity is positively evidenced by those who are fully recovering from massive strokes and other head traumas, overcoming learning disabilities, rehabiliting from obsessive-compulsive behaviors, erasing the pain of phantom limbs, restoring memory acuity and cognitive processing after injury, learning to react with ambient air disturbance without eyesight, practicing daily mediation to create lasting mind states of compassion and happiness, resuming the sympathetic nervous function for exercises after heart transplant, and on and on, but negatively by those who are abusing drug and sex, experiencing nervous control disorder and depression or even premature ejaculation or orgasm disorders. You get a bad habits without noticing the neuroplasticity. Neuroplasticity is for better or worse.
As described before, the brain possesses the remarkable ability to develop its nervous structure and function in response to a variety of internal and external stress, including repetitive behavioral training and relearning. Neuroplasticity allows the damaged brain to recover lost behaviors or abilities in response to rehabilitation by relinking or regrowing the damaged neurons and synapses. During brain repair following injury, the brain alternation is geared towards maximizing function in spite of the damaged brain. The undamaged brain cells surrounding the damaged area gear up their function and shape to take on the functions of the damaged cells. Studies show that astroglia, characteristic star-shaped glial cells in the brain and spinal cord are actively involved in the organizational and activational effects of sexual hormones and human growth hormone on synapse formation, synapse plasticity, and the response of neural tissue to brain injury. Sex hormones testosterone and estradiol promote astroglia differentiation and regulate astroglia gene expression for brain repair.http://recovery.tamu.edu/journal%20club%20articles/Garcia-Segura%201999%20astrocyt.pdf,http://www.strokestrategy.ab.ca/PDFs/JAK_neural_Plasticity.pdf
The effects of hypothalamus-pituitary hormones vasopressin, oxytocin and prolactin on neuroplasticity
Orgasm or high stress stimulates the hypothalamus to synthesize vasopressin, oxytocin and prolactin, and to force the pituitary gland to release them. Oxytocin gives you passion – loving and beloved feeling, enhances smooth-tissue(smooth-muscle) relaxation and expansion, and initiates orgasmic respones; prolactin gives your satisfaction and promotes tissue or muscle constriction and contraction; vasopressin facilitates psychological binding.
The brain evolution, as well as biological development of social behaviors, is affected by both genes and environmental stimuli. Studies have demonstrated that neurobiological substrates oxytocin and vasopressin play critical roles in modulating a wide variety of social behaviors, including social recognition, communication, parental care, territorial aggression, autism, and social bonding. Comparison of social behaviors across animal specie reveals that “differences in the density of receptors for oxytocin and vasopressin in ventral forebrain reward circuitry differentially reinforce social-bonding behavior in the two species. (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1764849/pdf/rstb20061939.pdf)” Both high levels of oxytocin receptor (OTR) in the nucleus accumbens and high levels of vasopressin 1a receptor (AVP1aR) in the ventral pallidum are responsible for monogamous social structure. Deplete oxytocin or/and AVP, or deficiency or depletion of of both receptors or genes will disturb or change the individual social behaviors, that is a process of life-term brain evolution. Studies shows Dopamine D2-like receptors in the nucleus accumbens seem to mediate social attachments by promoting Oxytocin and vasopressin secretion form the hypothalamus-pituitary axis .
http://carterlab.ucdavis.edu/courses/psc261/gingrich_liu_etal_BN2000.pdf,
http://www.ncbi.nlm.nih.gov/pubmed/8096618
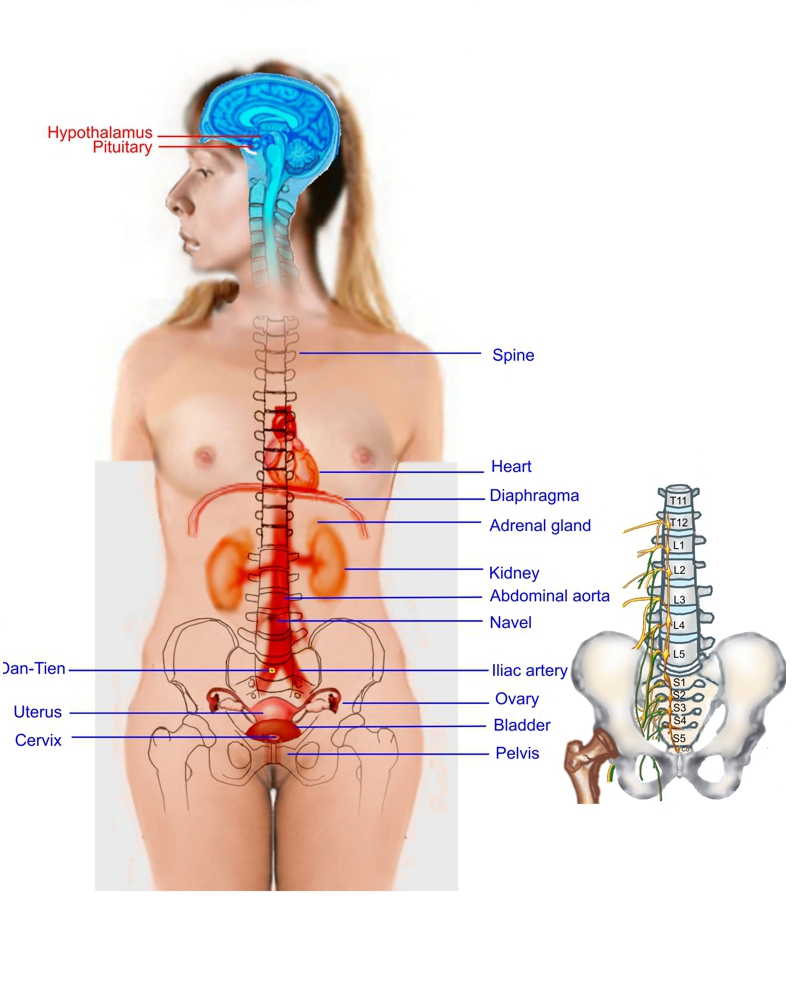
Vasopressin is also known as Arginine Vasopressin (AVP) which is well-known for promotion of water retention when body in dehydration state and for increase of arterial pressure while decreasing the kidney water excretion and increasing the kidney water reabsorption. The hypothalamus-pituitary axis produce and release three major hormones AVP, oxytocin and prolactin in response to extreme stresses, sexual stimulation and orgasm, leading to psychological and physiological alternation and mind state. The magnocellular cells in the supraoptic nucleus (SON) of the hypothalamus produce AVP and oxytocin; The parvocellular neurosecretory neuron in the paraventricular nucleus of the hypothalamus release vasopressin, corticotropin-releasing hormone (CRH), thyrotropin-releasing hormone (TRH), gonadotropin-releasing hormone (GnRH), growth hormone-releasing hormone (GHRH), and somatostatin (growth hormone release inhibiting hormone, GIH) into the blood vessels of the hypothalamo-pituitary portal system, which is a system of blood vessels that link the hypothalamus and the anterior pituitary in the brain. The neuropeptides are then carried to the anterior pituitary gland, where they are regularly release into the systemic circulation in response to stimulation. The parvocellular neurosecretory cells make the following hormones: corticotropin-releasing hormone (CRH), which stimulates the anterior pituitary gland to release adrenocorticotropic hormone (ACTH) by synthesizing from pre-pro-opiomelanocortin in response to biological stress ; AVP, which also regulates ACTH secretion (vasopressin and CRH act synergistically to stimulate ACTH secretion); Thyrotropin-releasing hormone (TRH), which regulates the secretion of thyroid stimulation hormones (TSH) and prolactin.
After being synthesized in the hypothalamus, AVP is stored in vesicles at the posterior pituitary to be released into the bloodstream; some of AVP is also released directly into the brain, where it exerts an biological effects on social behavior and bonding. Recent studies confirm that AVP affects memory formation, either long- or short-term, and neurpoplasticity in addition to social behaviors and physical water conservation balance in the body. Activation of the AVPr1a genes in the ventral pallidum which encodes pleasure or hedonic reward promotes pair-bond formation via a mechanism similar to addiction and reinforcement. Experiments shows that blocking the vasopressin receptors AVPr1a in the ventral pallidum ( http://en.wikipedia.org/wiki/Ventral_pallidum#Anatomy ) prevents any preferences or likening (http://www.jneurosci.org/cgi/reprint/25/38/8637 ), including sex partners, foods and so on. (http://jn.physiology.org/cgi/content/full/96/5/2175 . ) Studies shows vasopressin receptors distributed along the reward circuit pathway in the ventral pallidum are activated when AVP is released upon stimulation or social interaction, such as taste, olfactory sense, vision, hearing, mating or other stimuli. The activation of the reward circuitry reinforces this behavior, leading to conditioned partner preference and thereby to the formation of a pair bond. Sexually, the brain uses vasopressin as a reward for forming lasting bonds with a mate (http://www.jneurosci.org/cgi/reprint/21/18/7392 ); those who having one or two of the vasopressin receptor AVPr1a genetic alleles are likely to become promiscuous. Accordingly, peoples with one or two of the genetic alleles are more likely to have marital problems. Women with two of the alleles affecting vasopressin reception are likely to have a higher disappointing levels of satisfaction, affection, sexual pleasure, and cohesion.
Chronic over-masturbation in the early life over-stimulates the hypothalamus-pituitary-adrenal axis for excessive release of vasopressin, oxytocin, prolactin, norepinephrine, epinephrine and prostaglandgin E2
Upon stimulation, vasopressin and oxytocin release are increased from neurohornomal (or neurosecretory )cells in the pituitary glands. It also boosts the vasopressin and/or oxytocin biosynthesis in magnocellular cell nervous endings (somata). Prolonged activation of magnocellular neurons results in neuroplastic changes of cellular morphology , neurons, innervation pattern and synapses for chronic nervous deformation which produces psychological and psychiatric disorders and nervous or cellular inflammation. Eventually, the hypothalamus-pituitary function becomes very exhausted can fail to release an optimal amount of AVP, oxytocin and prolactin. This is why excessive sex or/and drug abuse, as well as excessive stress, in the early life produce a long-term consequence in later life, as a result of neuroplasticity.
Oxytocin is a passion or love hormone synthesized by the hypothalamus and released by the pituitary glands. The testosterone receptors and the dopaminergic nervous system are response for activating the hypothalamus-pituitary function to synthesize and to release oxytocin into the blood stream. Androgen hormones, including testosterone and dihydrotestosterone (DHT), can activate the dopaminergic nervous circuits for libido, sexual arousal and seeking reward. Except the self-stimulation and self-excitation inside the limbic system via fantasy thought or imagination, the external stimulation input from cranial sensory nerves are responsible for triggering the oyxtocin synthesis and release. The cranial nerves take five-sense stimulation input generated by kiss, touch, warmth, smelling, hearing, vision and/or affectionate expression. Note that fantasy thought or imagination is the 6th sense input to the hypothalamus-pituitary axis. Among the cranial nerves, the vagal nerve (CN-X) is longest one, projecting into the internal organs and the sex organs from the brainstem for modulation of the sympathetic nervous function via the oxytocinergic neurons, The vagal sensory nerve receives the stimulation input from the the internal organs, sex organs and skin-deep neuromuscular junctions in the front body. The vagal sensory nerve take sexual stimulation inputs from the breasts, nipples, abdomen, pubis, perineum, groins, penis, prostate, seminal vesicles, clitoris, vagina ( g-spot), cervix and uterus to the hypothalamus-pituitary axis for oxytcoin release. Oxytocin can cross the blood-brain barrier to act as a neurotransmitter in the oxytocinergic neurons which form synapses with other neurons in the forebrain, hindbrain, and spinal cord regions, and thereby modulate the central nervous system, cholinergic, parasympathetic and sympathetic nervous function in facilitating the dilation of the arteries in the brain and body. (http://www.ncbi.nlm.nih.gov/pubmed/6690342 ). In addition, oxytocin circulating in the blood steam as well as in the brain exerts its biological effects on its receptors to promote the arousal level of the nervous system and to increase the nervous sensitivity in the organs, particularly, the heart and sex organs. Oxytocin is released by stimulation from touch, kiss, warmth, emotional love auditory and visual stimulation, and affectionate expression. For example, sexual and breastfeeding stimulation on the vagal sensory nerves can trigger oxytocin release for orgasm. Oxytocin is responsible for expansion or dilation of smooth muscles and elastic tissues, particularly in the sex organs, heart, and nipples. Activation of oxytocinergic neurons increases extracellular dopamine in the nucleus accumbens and paraventricular nucleus of the hypothalamus for sexual motivation and reward, and evokes erectile function of smooth muscles.
During sexual arousal, the dopaminergic neurons in the in the nucleus accumbens and striatum are supposed to drive the pituitary oxytocin release, to fire up the oxytocinergic nerurons, and, then, to initiate the hypothalamus and adrenal dopamine-norepinephrine-epinephrine conversion mechanism in the stress response axis – the hypothalamus-pituitary-adrenal axis for the noradrenergic, adrenergic, sympathetic nervous activation. Here, activation of adrenergic ? receptors with epinephrine will facilitate the release of ?-endorphin, which modulates the cellular sensitivity of norepinephrine-induced prostaglandin E2 and histamine associated with inflammatory pains in the brain and sex organs and with premature ejaculation or orgasm. I have found that oxytocin elicits the binding of norepinephrine and epinephrine into the adrenergic beta receptors to facilitate smooth-muscle expansion, arterial dilation, erectile function, libido enhancement, and testicular function by increasing the blood flow into the brain and sex organs, which opposites the effects of its sister hormone prolactin that promotes the binding of norepinephrine and epinephrine into the adrenergic alpha receptors to facilitate smooth-muscle contraction, arterial constriction, limp erection, and ebbing libido. It allows the continuous stimulation of the testicular testosterone and DHT output which in turn keep the dopaminergic nervous activation during a sexual session. Once the oxytoninergic, NOergic (Nitric Oxide neuron), cholinergic (vagal and parasympathetic neurons)) and sympathetic nervous system (in its adrenergic beta receptors) maximizes the sex organ expansion, the hypothalamus-pituitary-adrenal axis in response to the extreme psychological and physiological stress in the sex organs initiates an abrupt dopamine-norepinephrine conversion and drops the dopaminergic action on the pituitary function, leading to release prolactin for smooth-muscle contraction and arterial constriction to bring the blood out of sex organs for mitigating the fullness of the sex organs. After the contraction is over, the stress response is mediated by oxytocin in the receptors; the hypothalamus-pituitary axis release the overflow oxytocin again to cause smooth-muscle expansion. The alternative pulsing of the prolactin and oxytocin release causes orgasmic contraction of the sex organs, brain, heart, arteries, and some organs with some smooth muscles or contractile tissues. Eventually, the prolactin effects become dominant, the smooth muscles return to flaccid state, and sexual arousal is over. The period of orgasmic contraction cycle, that is the prolactin-oxytocin release cycle, is about 0.8-second based up our measurement of the orgasmic vocal responses. This is my orgasmic theory.
http://content.apa.org/pubmed/bne/106/1/181
http://csbn.concordia.ca/Faculty/Pfaus/docs/Pfaus,Damsma,Nomikos,Wenkstern,%20Blaha,Phillips,Fibiger%20(1990)%20Brain%20Res.pdf
http://csbn.concordia.ca/Faculty/Pfaus/docs/Pfaus,Damsma,Wenkstern,%20Fibiger%20(1995)%20Brain%20Res.pdf
http://deepblue.lib.umich.edu/bitstream/2027.42/30731/1/0000380.pdf
http://www.sciencedirect.com/science/article/pii/S0018506X97914124
http://www.ncbi.nlm.nih.gov/pubmed/8402177
http://www.jneurosci.org/content/19/1/456.full.pdf+html
http://joe.endocrinology-journals.org/content/177/1/57.long
http://carterlab.ucdavis.edu/courses/psc261/gingrich_liu_etal_BN2000.pdf
http://www.ncbi.nlm.nih.gov/pubmed/17672853
http://www.nature.com/ijir/journal/v13/n3s/pdf/3900719a.pdf
http://www.elaine-m-hull.com/publications/testosterone_preoptic_dopamine.pdf
http://ajzenberg.com/dtae/manuscripts/campbell%20-%20Testosterone%20exposure,%20dopaminergic%20reward,%20and%20sensation-seeking%20in%20young%20men.pdf
http://www.elaine-m-hull.com/publications/effects_testosterone_metabolites.pdf
http://www.elaine-m-hull.com/publications/testosterone_restor_copulation.pdf
http://www.elaine-m-hull.com/publications/dopamine_medial_preoptic.pdf
http://www.elaine-m-hull.com/publications/effects_testosterone_copulation.pdf
http://www.psy.fsu.edu/faculty/hull/DA%265HT_pdf.pdf
http://www.elaine-m-hull.com/publications/hormone_neurotrans_sex_beh.pdf
http://www.psy.fsu.edu/faculty/hull/satoru_cGMP.pdf
http://balrog.wku.edu/~amaral/hormonas/estradiol02.pdf
http://neuro.cjb.net/content/22/21/9320.full
http://zlab.rutgers.edu/Integrative_NeuroSc/teachers/Morrell/article.pdf
http://www.psych.ucsb.edu/~roney/other%20pdf%20readings/reserve%20readings/sipos.pdf
http://linkinghub.elsevier.com/retrieve/pii/S0149763407001066
http://www.dafml.unito.it/anatomy/panzica/pubblicazioni/pdf/2006PanzicaNS.pdf
http://neuroscience.jhu.edu/Ball%20G%20Physiology%20Behavior%20.pdf
http://www.dafml.unito.it/anatomy/panzica/pubblicazioni/pdf/2008MartiniHB.pdf
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2001311/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2443938/
http://www.andrologyjournal.org/cgi/reprint/28/2/218
https://www.msu.edu/~sisk/publications/pdfs/paper3.pdf
http://www.psy.fsu.edu/faculty/hull/sato_NOS.pdf
http://www.psy.fsu.edu/faculty/hull/BR_getting_his_act.pdf
http://www.jurology.com/article/S0022-5347(01)62615-6/abstract
http://www.sciencedirect.com/science/article/pii/S0166432805003372
http://psycnet.apa.org/journals/bne/117/1/55/
http://psycnet.apa.org/journals/bne/112/5/1229/
http://onlinelibrary.wiley.com/doi/10.1111/1467-9450.00337/full
http://endo.endojournals.org/content/112/2/665.short
http://www.psychosomaticmedicine.org/content/61/3/280.full.pdf+html
http://www.ncbi.nlm.nih.gov/pubmed/11760788
http://www.ncbi.nlm.nih.gov/pubmed/15889301
http://66.199.228.237/boundary/Sexual_Addiction/orgasm_dopamine.pdf
http://joe.endocrinology-journals.org/content/186/3/411.full.pdf+html
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.19.4059&rep=rep1&type=pdf
http://www.ncbi.nlm.nih.gov/pubmed/15889301
http://www.ncbi.nlm.nih.gov/pubmed/11835982
http://www.ncbi.nlm.nih.gov/pubmed/15889301
http://www.ncbi.nlm.nih.gov/pubmed/15236835
http://www.ncbi.nlm.nih.gov/pubmed/11805404
http://www.ncbi.nlm.nih.gov/pubmed/17672853
http://www.ncbi.nlm.nih.gov/pubmed/17164075
http://www.ncbi.nlm.nih.gov/pubmed/16043278
http://www.ncbi.nlm.nih.gov/pubmed/9380788
http://www.ncbi.nlm.nih.gov/pubmed/9178353
http://www.ncbi.nlm.nih.gov/pubmed/8921295
http://www.ncbi.nlm.nih.gov/pubmed/21050872
http://www.ncbi.nlm.nih.gov/pubmed/16043278
http://ecmaj.ca/content/172/10/1327.full
Studies show that oxytocin plays an antinociceptive role in the brain via mu- and kappa-opioid receptors in the central nervous system. It calms the norepinephrine and sympathetic nervous function for anti-stress, well-being, social interaction, growth and healing. However, chronic elevation of oxytocin results in love or sex addiction, and romantic attachment. Divorce or separation produces love withdrawal symptoms, similar to opiate withdrawal. http://www.ncbi.nlm.nih.gov/pubmed/9924739?dopt=Abstract, http://www.ncbi.nlm.nih.gov/pubmed/15834840, http://www.ncbi.nlm.nih.gov/pubmed/15219651
Together, both oxytocinergic and vasopressinergic system promote pair bonding.
http://www.ncbi.nlm.nih.gov/pubmed/18655894
Oxytocin stimulates adult neurogenesis for neurogrowth and may protect against the suppressive effects of stress hormones on hippocampal plasticity. Chronic good sexual experiences can stimulate cellular proliferation and neurogenesis in the hippocampus.http://www.ncbi.nlm.nih.gov/pubmed/21692136 , http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2904381/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pubmed/18655894
http://www.ncbi.nlm.nih.gov/pubmed/21143653
Chronic physiological and psychological stimulation can cause AVP and oxytocin magnocellular neurons to experience the structural plasticity including the rearrangement of synapses, dendrites, and neurovascular contacts. http://www.ncbi.nlm.nih.gov/pubmed/20109532
http://www.ncbi.nlm.nih.gov/pubmed/18655878
http://www.ncbi.nlm.nih.gov/pubmed/18655888
Finally, serotonin can excite the magnocellular neurons via multiple receptor subtypes and mechanisms to promote the release and the gene expression of vasopressin and oxytocin in the hypothalamic paraventricular nucleus.
http://www.ncbi.nlm.nih.gov/pubmed/17561813
Prolactin is a cytokine hormone synthesized in the hypothalamus and released by the pituitary during peripartum, breastfeeding and orgasm or in response to stress, to facilitate muscle contraction and arterial constriction. It also acts as neuromodulator and regulator of neuronal and glial plasticity in the brain. Prolactin induces neuroplasticity via a gene Egr-1 mRNA expression located in the oxytocinergic neurons of in the hypothalamic paraventricular (PVN) and supraoptic nuclei (SON). It affects the nervous system on multiple levels: prolactin promotes neurogenesis, neuronal survival after stress in the hippocampus, and the differentiation of neurospheres into mature neurons, and is capable of repairing myelin damage by increasing oligodendrocyte numbers, myelin basic protein and myelinated axons. Note that prolactin has been identified as a potential therapeutic agent for multiple sclerosis because it remits multiple sclerosis during pregnancy. Prolactin can cross the blood-brain barrier via a transport system in the choroid plexus to exert its biological effects on its receptors in several brain regions including the hippocampus and the paraventricular (PVN) and supraoptic (SON) nuclei of the hypothalamus and on its cytokine family receptors for either inflammation (if excessive, prolonged stimulation) and neurogenesis and calmness (if optimal release), and to activates the mitogen-activated protein (MAP) kinase cascade and Egr-1 gene expression in the hypothalamus for vascular endothelial growth factor and plastic change of hypothalamus. The induced neurplasticity includes glial retraction and remodeling of synaptic contacts of oxytocinergic neurons. A high level of prolactin in the brain will mimincs maternal behavior and inhibit the hypothalamic -pituitary-adrenal and -ovarian axis during lactation by stimulating the hypothalamic PVN and supraoptic nucleus.
http://www.ncbexert on inhibitation effect oi.nlm.nih.gov/pmc/articles/PMC2783212/pdf/nihms146333.pdf,
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2659278/?tool=pubmed
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2659278/?tool=pubmed
Prolactin stimulates the secretion of oxytocin and AVP under the regulation of nitric oxide in PVN and SON. However, the pituitary prolactin secretion is regulated by neuroendocrine neurons in the hypothalamus. The prolactin secretion is inhibited by the activation dopamine D2 receptors of the the tuberoinfundibulum (TIDA)dopmaine neurons in the arcuate nucleus of the mediobasal hypothalamus. On the other, thyrotropin-releasing factor (thyrotropin-releasing hormone), produced by the hypothalamus in medial neurons of the paraventricular nucleus, stimulates the release of thyroid-stimulating hormone and prolactin by the anterior pituitary. http://www.ncbi.nlm.nih.gov/pubmed/20943859
http://www.sciencemag.org/content/299/5603/117.abstract?ijkey=5d2af93ba3b52124b33066390c68af42856858b8&keytype2=tf_ipsecsha,http://www.jneurosci.org/content/27/8/1812.full.pdf+html
On the other hand, elevated serum prolactin has been associated with autoimmune disease and cancers. A high level of serum prolactin in the blood stream is called hyperprolactinemia. Prolactin stimulates cellular proliferation and differentiation, and contributes to pathogenesis and chemoresistance of breast cancer and prostate.
http://www.ncbi.nlm.nih.gov/pubmed/21726627 , http://www.ncbi.nlm.nih.gov/pubmed/21719533 http://www.ncbi.nlm.nih.gov/pubmed/16249247, http://endo.endojournals.org/content/149/10/4821.full.pdf+html http://rheumatology.oxfordjournals.org/content/45/1/97.full.pdf+html
http://www.ncbi.nlm.nih.gov/pubmed/21688280
Prolactin is also known as the lactation hormone since it stimulates the ammary glands to produce milk under nipple suction. A high progetserone level during pregancy normally inhibits milk production. after the end of pregnancy. the drop of placenta progesterone, in conjunction with nipple suckling stimulus, will initiate milk production. Prolactin counteracts the dopaminergic and oxytopcinergic action on the hypothamalus-pituitary-adrenal and -testicular (-ovarian) axis. There is an increase in serum concentrations of prolactin during pregnancy, resulting in cooling down the hypothamalus-pituitary-adrenal axis, in blocking the hypothamalus-pituitary-ovarian axis, and in inhibiting orgasmic responses.
The pituitary oxytocin release under the dopaminergic action, in conjunction with hypothalamic and adrenal dopamine-norepinephrine conversion promotes libido and sexual desires. After orgasm, the dopaminergic action ebbs for the pituitary gland to release prolactin for cooling down the norepinephrine and sympathetic nervous system. Thus, prolactin gives the body sexual gratification after sexual orgasm. Some studies proposed that the amount of prolactin release serves as an indicator for the amount of sexual satisfaction and relaxation. The problem is that if sexual arousal or stimulation result in excessive prolactin release for an exhausted hypothalamus-pituitary-adrenal axis, the erectile function and libido will go limp. In this regard, the amount of prolactin becomes an indicator of sexual dysfunction This is because prolactin counteracts the effects of dopamine and oxytocin on sexual arousal and arterial dilation. Elevation of prolactin and norepinephrine after orgasm also causes arterial constriction that restrict the blood blow to the brain and sex organs and disables sexual functions immediately for both men and women. If the dopaminergic, oxytocinergic and NOergic nervous action can overcome the arterial constriction, prolactin in the bloodstream can enhance the response of Leydig cells to luteinizing hormone (LH) by increasing the number of LH receptors, resulting in testosterone secretion and leading to spermatogenesis. This may explain why orgasm can increase the testicular testosterone and DHT secretion for some people, but why it can exhaust the hypothalamus-pituitary-adrenal and testicular (or -ovarian) axis for others. Those who can have multiple orgasms in one love session don’t experience a significant elevation of prolactin during sex. However, the gradual elevation of prolactin after each orgasm will diminish their sexual potency and orgasmic function. A drop of the pituitary prolactin release in the post-orgasm state will help people to restore the sexual power. The time for sexual recovery is termed as the refractory period. A unusually high amount of prolactin is responsible for inhibition of the ovarian and testicular function, impotence, orgasmic dysfunction, loss of libido, and loss of the menstrual cycle in lactating women as well as lactation-associated osteoporosis.
Coping Stress or meditation can stimulates hippocampal neurogenesis for a recovery of neuroplasticity As long as you can reduce your hypothalamic and adrenal dopamine-norepinephrine conversion, you can return your mind and consciousness to your innocent state.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2930418/?tool=pubmed, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2671071/pdf/nihms99452.pdf